Decompression sickness
Even though diving accidents are thankfully very rare, it is important to know the factors that contribute to them occurring. This is the only way that we can take a targeted approach to keeping the risk of a decompression accident low, recognising early signs and starting appropriate treatment.
Symptoms of a DCS
Decompression sickness (DCS) is any condition that arises as a result of an excessive accumulation of nitrogen in the tissues. It is caused by the formation of gas bubbles during the decompression phase (i.e. during surfacing) and after the dive on the surface. We differentiate between mild DCS symptoms and serious DCS symptoms. Currently, any symptom that is more severe than unusually increased tiredness and itching (so-called "creeps") are seen as indications of serious decompression sickness.
As gas bubbles can develop in various tissues, a variety of symptoms can arise.
With decompression sickness of the skin, bluish-red discolourations develop that appear streaky or blotchy ("marbled") and are often painful. These particularly develop on fatty body parts, such as the abdominal skin, the sides, the upper arms or the thighs. In women, breasts may also be painfully swollen.
DCS of the muscles and joints manifests as pains, particularly in the large joints, i.e. shoulders, hips or knee joints. The pains often develop on both sides. Typically, there is a persistent stabbing or tearing pain in the affected joints.
A large volume of bubbles in the blood vessels leading to the heart can make it more difficult for blood to flow to the lungs. Affected divers complain of shortness of breath.
Air bubbles can form directly in nerve tissues but can also be carried in the blood stream to the central nervous system arteries, where they can cause symptoms similar to a stroke. In this case, various neurological symptoms are possible. These range from symptoms of dizziness, often associated with nausea and vomiting, tingling in the arms and legs, hemiplegia and paraplegia, drowsiness to loss of consciousness.
Basic principles
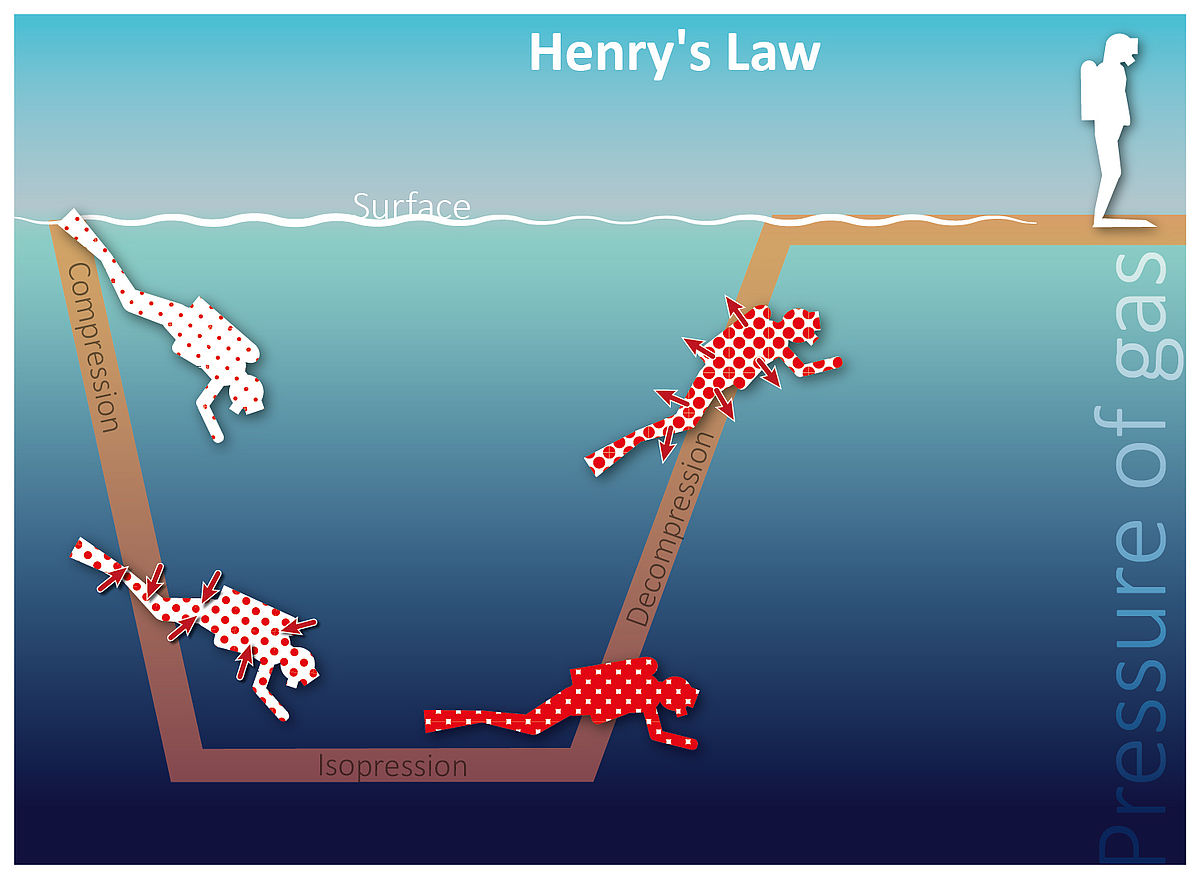
As our breathing air is mainly composed of nitrogen, each dive leads to our tissues becoming saturated with this gas – which is completely harmless on the surface of the water. The amount of nitrogen absorbed by the tissues depends on various factors. According to Henry's law, gasses dissolve in liquids. The higher the gas pressure, the more gas is dissolved. This process takes a certain amount of time. For us divers, this means: the longer and deeper we dive, the more nitrogen is dissolved in the blood. Via the blood, nitrogen enters the tissues, which absorb nitrogen more quickly the more they are supplied with blood.
Different tissues can absorb a completely different amount of nitrogen before they are "saturated". When surfacing, the different tissues therefore also release the nitrogen at different rates.
As each diver is different in terms of body composition and fitness (and therefore in terms of blood flow to the individual tissues) and also in terms of certain pre-existing illnesses and risk factors, each individual has their own risk of suffering DCS. In addition to infections and febrile illnesses, chronic illnesses such as diabetes, high blood pressure, obesity or an overactive thyroid can have a strong effect on nitrogen absorption. Other risk factors could be smoking, excessive alcohol consumption on the previous day, dehydration, old age, stress, tiredness and also (minor) injuries, sunburn or severely aching muscles. Put simply: every diver has a different individual risk! This also depends on their condition on the day. No dive computer in the world can take these factors into account as it doesn't know you – and therefore doesn't know your individual factors. Here, it is a good idea to adjust the settings of the dive computer ("conservatism" or "micro bubble level") in accordance with your own, individual risk. In doing this, you should consider your own risk factors very (self-)critically.
Furthermore, in addition to the period and the depth of a dive, other factors that are specific to the dive may affect the absorption of nitrogen. Physically and emotionally strenuous dives, e.g. diving in strong currents or under stress, promote the accumulation of gases in the tissues. Of course, the dive profile, the number of repeat dives, the length of surface intervals between the individual dives and the breathing gas used all play a role.
The rate at which the nitrogen is released also depends on several factors. The more nitrogen is absorbed by a tissue and the quicker the pressure falls (i.e. the quicker the rate of ascent), the greater the supersaturation of the tissue. The better the blood flow to a tissue, the quicker the release of the nitrogen into the blood. However, nitrogen does not stop being released when you reach the surface. The slower tissues (i.e. those with worse blood flow) also continue to release nitrogen even several hours after the dive so that the amount of gas bubbles circulating through the body is at the highest approximately two hours after the dive. These bubbles are retained in the lung capillaries as in a large filter and slowly get smaller as the nitrogen leaves the bubbles and is released via the air sacs when you breathe. A large amount of bubbles can block the circulation of the lungs and cause shortness of breath. This places severe stress on the cardiovascular system. In order to relieve stress on the heart, shunts can open up in the lungs. Via these so-called lung-shunts, gas bubbles can pass to the body's circulation where they can cause circulatory problems in the tissues. Depending on where this happens, very serious clinical pictures can arise, such as an arterial gas embolism in the brain, which is similar to a stroke.
Via these so-called lung-shunts, gas bubbles can pass to the body's circulation where they can cause circulatory problems in the tissues. Depending on where this happens, very serious clinical pictures can arise, such as an arterial gas embolism in the brain, which is similar to a stroke.
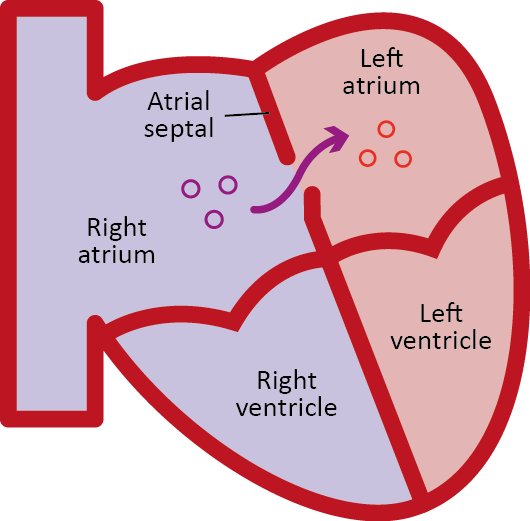
The persistent foramen ovale, a hole between the cardiac atria which exists in one in every three or four adults as a remnant of the circulatory system when they were in the womb, can also lead to bubbles passing from the veins into the arteries.
Prevention
In contrast to a couple of years ago, diving medicine now assumes that gas bubbles form during each dive. How many depends on individual and dive-specific factors. The only way in which you can be 100% sure to avoid decompression sickness is therefore not to go diving! However, the risk can be reduced significantly by sensible behaviour both during and after the dive.
Before diving, each diver should critically assess themselves, their state of health and fitness and their level of stress and fluid balance. Am I physically fit enough for the planned dive? Have I had enough training and is my equipment suitable? These questions can help you to reduce stress during the dive itself. If in doubt, it may be better to plan a more conservative dive or even to skip a dive.Optimum preparation also includes the individual setting of the dive computer and choosing the correct breathing gas. The use of nitrox can help to reduce the amount of nitrogen that accumulates in the tissues during the dive. For increased safety, it is important to note that the dive computer must remain set for compressed air and NOT for nitrox. Otherwise, the no-decompression limit will be calculated based on the lower amount of nitrogen and will therefore be considerably longer. A correspondingly longer dive using nitrox would result in the same DCS risk as a shorter one with compressed air.During the dive, every diver should stick to their plan responsibly. This could be discussed with the dive guide in advance if necessary (e.g. "I'm not very physically fit so I would prefer to do a more shallow dive"). Yo-yo profiles, i.e. a new descent after starting to surface, should be avoided at all costs. In any event, it is important to control the rate of ascent. The more shallow the dive depth during ascent, the sharper the relative decrease in the ambient pressure; therefore, even after the safety stop, you should surface very slowly for the last few metres at the end of the dive. Of course, prescribed safety or decompression stops must be observed. It wouldn't hurt to extend these stops somewhat, particularly in more shallow areas.
There is also lots that you can do after a dive to reduce the risk of decompression sickness.
As everything that increases blood flow to the tissues causes an accelerated release of nitrogen, you should not be exposed to intense heat for the first few hours after diving. As tempting as it may be when you emerge from the water feeling cold, do not sunbathe, have hot showers or use a sauna directly after diving. You should even refrain from taking part in sports or having a massage shortly after a dive. There is no definitive recommendation of how long you should wait. The period depends on body composition, the duration, depth and stress during the dive and various individual factors. It is best to undertake light sports activities in the morning before diving, but you should avoid trying to achieve peak performances and losing large amounts of fluids. Save the sauna for a day when you are not diving. Alcohol also promotes blood flow to the tissues by widening blood vessels. You should therefore wait for a certain period of time after diving before having your deco beer.
As shunts form in the lungs for all of us in certain circumstances allowing bubbles to enter the arterial circulatory system, you should avoid any activities that would cause increased pressure in the chest directly following the dive when there is a high level of bubbles. This particularly happens with heavy lifting, but also when coughing, pushing, blowing up air beds etc. Occasionally, it may lead to an increase of pressure inside the lungs if it is difficult to get into the dinghy. There is a simple solution to this: diving is, after all, a buddy sport! Lots of strenuous activities, such as carrying heavy equipment, is much less strenuous with two people and therefore only causes a slight increase of pressure in the chest. This allows the transfer of nitrogen bubbles from the veins into the body's circulation system to be significantly reduced.
It goes without saying that you shouldn't get on an aeroplane directly after diving. The drop in atmospheric pressure can cause existing gas bubbles in the blood or arteries to get even bigger and lead to complications. Of course, this doesn't only apply to air travel! Even travelling over mountain roads or visiting nearby mountain regions can lead to further decompression, i.e. a decrease in pressure, and therefore to a greater relative level of tissue saturation and an increase in size of existing bubbles. It would therefore be better to plan a separate holiday for paragliding and mountain hiking.
It is important to observe a sufficiently long surface interval with repeat dives. If a large amount of nitrogen bubbles are still travelling through the blood vessels, these get smaller during a repeat dive and can then pass through the lung capillaries. During a repeat dive they then re-expand so that there is now also a large amount of bubbles in the arterial system! A repeat dive during the period when there is a high level of bubbles would therefore have the same effect as a yo-yo dive. Surface intervals should be as long as possible, particularly after challenging dives. A rest of three hours or more is recommended. After deco dives, challenging technical dives or if there is a high individual risk (divers with a known PFO, divers with diabetes, older divers etc.), no repeat dives should be undertaken at all.
Treatment
The current Diving Accident Guidelines for treating decompression sickness have been available since 2014. Particularly with mild symptoms and ambiguous complaints, it is important to first consider the possibility of DCS. We assume that even creeps and tiredness are rarely recognised as indications of decompression sickness. Even with muscle and joint pain or blotchy skin, another explanation can readily be found: DCS? Isn't that something that other people get?
There are two important principles for treatment: giving oxygen, which helps to shrink any gas bubbles; and giving fluids. If there are mild symptoms and the diver is conscious and can swallow, fluids should be offered as drinks - approximately half a litre to one litre per hour. Any drink is suitable for this; only alcohol should be avoided. If the symptoms are only mild, the diver can be observed. With oxygen, more is more!

Demand or Wenoll systems are therefore ideal as these can supply 100% oxygen. Free-flowing oxygen should be given using a mask with a reservoir bag and with the highest possible flow rate of 15 l/min. Nasal cannulas or probes are not as well suited as these only allow a lower concentration of oxygen in the inhaled air. If this is the only available system at the scene of the emergency, this is still much better than not giving any oxygen.
Attention should be given to any neurological symptoms that may arise, such as disturbed sight, hearing and speech, numbness or paralysis. A set scheme is the most appropriate method for carrying out regular checks, such as the so-called 5 Minute Neuro Exam. This scheme should be carried out repeatedly and the results should be documented together with the time. If mild symptoms disappear within 30 minutes of treatment, a doctor should be informed for further checks and the diver should be observed for a further 24 hours. If there are still symptoms, treatment is continued. Contact is made with the nearest diving doctor or the nearest decompression chamber via the rescue coordination centre, the diving base or the divers' emergency service.
If loss of consciousness occurs where there is suspected decompression sickness, the diver must be put in the recovery position. In the event of a cardiac arrest, the patient must be placed on their back and CPR should be started immediately. At the same time, other helpers should notify the emergency services (112 or 911). The diving base, rescue coordination centre or divers' emergency service will inform the decompression chamber. CPR should be continued until the emergency services arrive. If possible, oxygen should be given at 100% using mask ventilation. Only experienced and appropriately trained helpers should give any intravenous infusion solutions.

Summary
Nitrogen is absorbed by the tissues during each dive. During surfacing and after the dive, nitrogen is released back into the blood; bubbles form.
The quicker the decrease in ambient pressure, the larger the bubbles and the greater the amount of bubbles are formed. Good self-assessment, a clean dive profile and acting wisely after the dive help to keep the risk low.

