Sickle-cell anaemia
A rare condition for dive doctors, caring parents and interested divers:
Sickle-cell anaemia
What do Tabea, Mike, Yasmin, Joshua and Karim have in common (names have been changed by the author)? They are between 11-34 years old, grew up in Germany and want to become divers. However, they also have another thing in common: their genetic material does not originate from Europe.
Karim has Iranian parents though born in Germany. Mike and Joshua were adopted as babies from German parents but are originally from Africa (Uganda, Congo). Yasmin was also adopted, but born in Pakistan. As a child, Tabea came with her parents from Tanzania to Germany and is now an anesthesiologist.
All of them can swim and feel comfortable in the water. All look healthy and are more or less physically fit. That basically sounds like a normal person. And yet, something is special about their needs in a fitness to dive examination: it is their genetic heritage from countries which are geographically close to the Equator. Countries where Malaria is endemic – and in which the so-called sickle-cell anaemia occurs frequently.
What is sickle-cell anaemia?
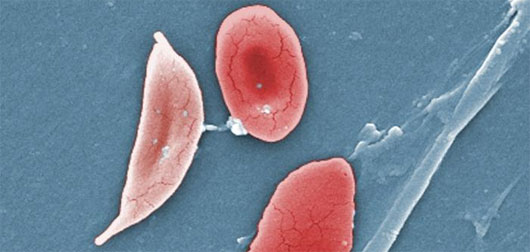
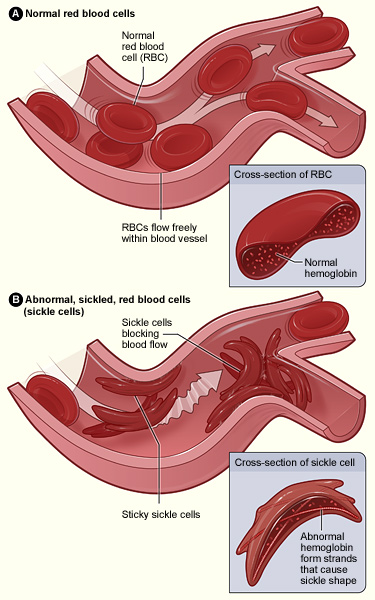
Sickle-cell anaemia is a genetic disease. Due to a genetic defect, the haemoglobin – one component of red blood cells – is produced in an abnormal way. As a result, the red blood cells are crescent-shaped. Sickle-cell anaemia is one of the so-called "hemolytic anaemias", which means that the red blood cells do not reach their normal life span of 120 days. Consequently, people with sickle-cell anaemia suffer from fatigue, a loss of power and energy and are more susceptible to infections. These are the usual symptoms when suffering from anaemia. In case of sickle-cell anaemia, there is an additional issue.
The crescent shape of the erythrocytes can lead to an obstruction in capillaries resulting in a restriction of the blood flow to an organ. This complication usually occurs during a so-called sickle-cell crisis, when suddenly a lot more red blood cells change their shape at the same time and are caking or clumping.
Triggers for such a vaso-occlusive crisis are, for example, a lack of oxygen (due to high altitude, lung diseases, narcosis), physical exertion, a cold climate, infections or inflammation. Due to the restricted blood flow and the malperfusion, silent or unnoticed repeated sickle-cell crises can lead to serious long-term damage in organs (brain, lung, eyes, kidneys, spleen, etc ... ). In addition, a sickle-cell crisis is very painful. The patient suffers from severe pain that is usually located in the abdominal or chest area and / or in the joints.
The genetic disease is inherited in an autosomal recessive pattern, meaning regardless of the sex chromosomes x and y. Chromosomes always come in pairs – one from each parent. If a child receives one healthy and one sick chromosome (heterozygous form), the haemoglobin will be partly normal (HbA) and partly abnormal (HbS), more or less in the ratio 1:1. The heterozygous form (sickle cell trait) is almost always asymptomatic and people only get ill when triggered by certain factors (lack of oxygen, cold, exertion, infections, etc. ... ). If a person is a homozygous carrier with two abnormal chromosomes, the haemoglobin is exclusively HbS formed. Even normal physiological conditions can trigger a deformation of the red blood cells. Sickle cells snag easily and lead to the above mentioned complications.
Now back to Tabea , Mike, Yasmin, Joshua and Karim. Why should we check for sickle-cell anaemia in their fitness to dive examination and not in other people's examinations?
Sickle-cell anaemia has the largest prevalence in regions of Africa and Asia where there is a high rate of malaria – exactly where the genetic material of those five diving aspirants originates from.
In Equatorial Africa, 25-40 % of the population are heterozygous carriers of the trait. The frequency of the defect decreases significantly the greater the distance from the equator. Within the black population in America, the prevalence drops down to 5-10 %. This phenomenon can be explained by the fact that heterozygous carriers have a relative resistance to falling sick with malaria. This constitutes a significant selective advantage in malaria regions, which is not necessary in moderate latitudes.
So at least one good thing comes from this disease – a relative resistance against malaria.
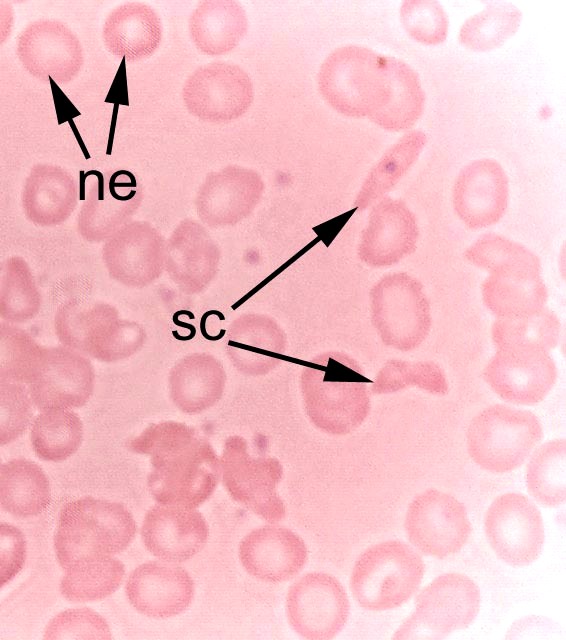
Diagnosis: A good indicator is the family history. If a blood relative has been diagnosed with sickle-cell anaemia, one should get tested. The final diagnosis is made by laboratory tests based on a complete blood cell count (presence of so-called target cells) and should be additionally supplemented by a special sickle cell test (haemoglobin electrophoresis restriction analysis).
What does all of this have to do with diving and the fitness to dive examination?
Even in a warm climate and during the most relaxing diving holiday, cold and exertion, possible infections, physical stress and dehydration are constant buddies of a diver. Therefore, the common triggers for sickle-cell crises are always on board. It is not 100 % known how the sickling of red blood cells – as the main transporters of oxygen – affects the saturation and de-saturation of nitrogen during a dive, but one expects a disadvantageous alteration.
Homozygous carriers (2 abnormal chromosomes) are therefore strictly excluded from diving. In heterozygous carriers, who are otherwise healthy in everyday life, the result of the sickle cell lab test is crucial. If the erythrocytes take the crescent form during oxygen deprivation, we don’t recommend diving.
If the cells keep their normal shape, one still has to educate the potential diver about the health risks even while diving in restricted limits. Diving in cold water, ice diving and strenuous dives (e.g. rescue and salvage missions) should be avoided. Professional divers and children under 18 are note rated fit to dive in this case.
In case of sickle-cell anaemia, the fitness to dive examination should be repeated every year regardless of age. Beside the normal examinations and tests, the dive doctor will decide about additional features according to the present symptoms (ultrasound of abdomen and heart, eyes, kidneys, etc. ...)
In Germany, about 300 children and adults are affected by sickle-cell disease each year. Most of them are immigrants from malaria endemic areas – or adopted children / adults. Overall, the sickle-cell anaemia is not a very common problem in a dive medical ambulance. However, the dive doctor should be aware of it in particular cases and it does not hurt if the dive centre asks about it when dealing with according people.

